This supplement is one part of my broader evidence-based stack. If you’d like to see how all the pieces fit together, and how I rank them by research strength, you can explore the full list here.
Vitamin D3 sits at the intersection of sunlight, metabolism, and skeletal integrity. It is not a novelty supplement. It is a hormone precursor with wide systemic effects. The question is not whether Vitamin D matters, but whether supplementing D3 improves outcomes beyond diet and sensible sun exposure.
Which test to order: 25-hydroxyvitamin D [25(OH)D]. Do not use 1,25-dihydroxyvitamin D except in specific renal or calcium disorders.8
Target range: Reasonable functional target for most adults: 20–50 ng/mL (50–125 nmol/L). Some groups aim a bit higher; avoid chasing extremes.
Fasting & keto context: Absorption improves with fat. If you alternate-day fast, as I do, consider dosing with eating windows.
Form:D3 (cholecalciferol) is preferred to D2.
Pairings: Magnesium sufficiency supports vitamin D metabolism. K2 pairing is biologically plausible for calcium handling; clinical evidence remains limited.9
Final Verdict
Vitamin D3 is worth taking when deficiency risk is present or confirmed. It is foundational for bone health and plausibly supportive for immunity and overall resilience, especially in those starting low. Treat lab values, over headlines.
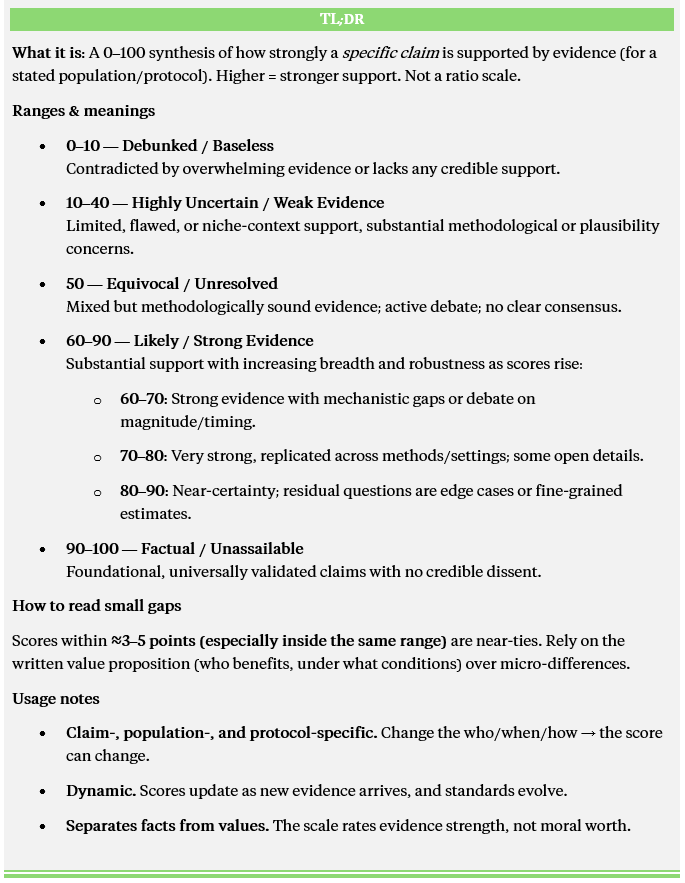
Final ETCS Score for Vitamin D3: 82/100
Here’s a quick ETCS breakdown → full explanation here. Hat tip to George Michaelson for encouraging me to clarify the model.
…
If you found this helpful, let’s keep the conversation going:
Subscribe for more evidence-based deep dives on health, longevity, and performance.
Share this post if someone you know is navigating D testing or dosing.
Vitamin D3, when taken as a supplement, is well established to raise blood levels of 25-hydroxyvitamin D (25(OH)D), which is the form measured to assess vitamin D status. This rise is consistent across healthy adults and those with deficiency, with more marked increases seen in people starting with low baseline levels. Deficiency in vitamin D impairs the body's ability to absorb calcium, leading to bone demineralization (weakening of bone structure) and, over time, increased risk of fractures or osteoporosis. In people who are deficient, supplementing with D3 reliably prevents or reverses bone loss, improves bone mineral density, and lowers fracture risk, especially when combined with adequate calcium intake. People with normal vitamin D status do not see further bone benefits from additional supplementation, but for those whose blood levels are low, D3 is one of the best-evidenced ways to restore bone health.
Vitamin D3 plays a crucial supporting role in the prevention of fractures and the maintenance of bone density, especially when paired with calcium. In older adults, particularly those who are frail or living in care settings, the evidence is clear: regular doses of vitamin D3 together with adequate calcium modestly lower the risk of fractures, including hip fractures, which are one of the most significant threats to independence in later life. Alone, D3 supplementation is less consistent for fracture prevention, with large trials and meta-analyses generally finding that D3 by itself does not reliably reduce fracture rates, except perhaps in those who start off severely deficient. However, D3 (with or without calcium) reliably supports bone mineral density in people who are vitamin D deficient, reinforcing the principle that adequacy matters most and that benefits level off once sufficiency is reached. The “dose makes the medicine,” as high-dose D3 by itself can sometimes backfire, and mega-doses are not recommended. For best results, pair daily vitamin D3 (around 800 IU) with calcium (about 1000–1200 mg), especially if there are risk factors for deficiency or frailty.
Vitamin D3 offers a modest but real shield against respiratory infections, especially for people whose vitamin D levels are low to begin with. Large, high-quality meta-analyses and systematic reviews show that the strongest benefits appear in those who are clearly deficient, sometimes slashing infection risk by half in this group. Taking D3 daily or weekly (at typical doses of 400–1200 IU per day) works better than taking large, infrequent “bolus” doses. In studies, people who took regular, moderate doses had fewer colds, cases of flu, and other respiratory illnesses than those taking big doses every month or less often. If vitamin D levels are adequate, extra doses probably do little, but for the many who are low, especially in winter, or in older age, or with limited sun, supplementation is a safe, practical safeguard. The protective effect is best described as “modest”: the number needed to treat to prevent one respiratory infection can range from 10 to 36, depending on baseline status and dose regimen. Mechanistically, vitamin D supports immune signaling and antimicrobial defenses, but does not act as an all-purpose cure.
Vitamin D3 plays a background role in mood and cognition, but its effects are subtle and situational. Observational research often finds people with low vitamin D levels are at higher risk of depression or low mood, but causality is tricky: factors like staying indoors, poorer health, or less social engagement may explain both low D and low mood. When it comes to supplementing, large meta-analyses of randomized controlled trials show that D3 can produce small improvements in depressive symptoms, particularly when correcting a clear deficiency. However, these effects are often minor and more evident in people with baseline low D or clinical depression rather than healthy individuals. For cognitive function, similar nuances hold: randomized trials in older adults and people with mild cognitive impairment or Alzheimer’s found some positive effects of D3 supplementation on memory and attention if deficiency was present, but healthy adults or those starting with normal D levels show little consistent benefit. In the largest, longest studies, D3 does not work like an antidepressant or cognitive enhancer for the general population. It may be helpful if you’re too low, and neutral if you’re already sufficient.
Vitamin D3’s effect on reducing all-cause mortality, cardiovascular disease (CVD), or cancer risk is complex and context-dependent. Large high-quality randomized controlled trials and meta-analyses have yielded mixed outcomes overall. While some meta-analyses find a modest reduction in all-cause mortality associated with vitamin D supplementation (about 7% lower risk in one large review), these benefits are more pronounced in subgroups with low baseline vitamin D levels rather than the general population. Regarding cardiovascular disease, despite observational links between low vitamin D status and greater CVD risk, the strongest evidence from large, well-powered RCTs shows no clear protective effect of vitamin D supplementation against heart attacks, strokes, or heart failure when given to the general adult population. Cancer incidence does not appear reduced by vitamin D supplements, but some studies suggest a possible decrease in cancer mortality, particularly for certain cancers, though this remains an area where more research is needed. So, treating vitamin D deficiency is important and may reduce health risks in deficient individuals, but population-wide supplementation without deficiency appears unlikely to lower mortality or major disease risks significantly. Focus on correcting deficiency first and maintain realistic expectations for broader benefits.
Vitamin D3 toxicity is uncommon but can occur if very high doses are taken over a prolonged period. The main risk is hypercalcaemia, a condition where calcium levels in the blood become too high, which can lead to symptoms like nausea, weakness, and kidney problems. Blood tests measuring serum 25-hydroxyvitamin D can help detect this, with levels above approximately 150 ng/mL (about 375 nmol/L) serving as a practical warning sign of potential toxicity. Most people taking typical supplementation doses (up to 4000 IU daily) stay well below harmful levels, so monitoring should focus on those using very large doses or with conditions affecting calcium metabolism.
Certain health conditions require extra caution with vitamin D3 supplementation because they can increase the risk of harmful side effects, particularly related to calcium balance in the body. If you have sarcoidosis or other granulomatous diseases, your body may produce excess active vitamin D, raising calcium levels dangerously high even without large supplements. Similarly, people with primary hyperparathyroidism have an overactive parathyroid hormone, which also disrupts calcium regulation, creating risk if vitamin D3 is supplemented without medical oversight. Advanced chronic kidney disease (CKD) affects the kidney’s ability to process vitamin D properly, so dosing must be carefully managed. Additionally, thiazide diuretics, which are a common blood pressure medication, reduce calcium excretion by the kidneys, potentially compounding vitamin D-induced hypercalcaemia risk. If any of these apply, it’s important to coordinate vitamin D supplementation with healthcare professionals who can monitor calcium and vitamin D status regularly to avoid complications.
Magnesium is essential for vitamin D metabolism, acting as a foundational co-factor that supports the enzymes responsible for producing active vitamin D in the body. If magnesium is low, the body may struggle to efficiently convert vitamin D into its usable form, making sufficiency a practical prerequisite when optimizing vitamin D status or correcting deficiency. For most, typical dietary intake is adequate, but for those with low intake or high calcium-to-magnesium ratios, magnesium supplementation may be warranted. Combining vitamin D3 with vitamin K2 is biologically plausible for improved calcium management. Vitamin D3 increases calcium absorption, while K2 helps guide this calcium into bones and teeth, rather than allowing it to deposit in soft tissues like arteries or kidneys. Experimental and animal studies support this synergy, but in humans, clinical evidence for benefit is less robust so far. Some trials and meta-analyses suggest that K2 supplementation can help maintain bone mineral density and might reduce fracture risk in certain populations, especially postmenopausal women, but consistent, high-quality randomized trial evidence is still emerging.